In Support of e-Cigarettes as a Substitute for Tar-Containing Tobacco Cigarettes

C-rations, battle field necessities
As a recent convert to e-cigarettes I made a simple test to satisfy what I had known since I was a teenager. If you inhale on a tobacco cigarette and exhale through a white paper towel you can see the brown tar residue on the paper. If you do the same test with an e-cigarette there is no visible residue.
I am pleased to know that what I inhale does not contain the carcinogenic tarry components of traditional cigarettes. Non-filtered cigarettes, which I smoked for years, carry even more tar. E-cigarettes are controversial because they are new, and – well, they are called cigarettes. There is confusion about what e-cigarettes are. This link should clarify what we are talking about.
That tobacco cigarettes are harmful is beyond dispute. My grandfather played the French horn and smoked non-filtered cigarettes for over 50 years and died from a fall down steps. Tobacco cigarettes are, then, mildly toxic with prolonged use (as opposed to highly toxic cyanide or Zyklon B).
Second-hand tobacco smoke has been shown to be harmful as well, although used tobacco smoke must be less toxic than freshly inhaled tobacco smoke, we must take into consideration of other sources of second-hand smoke.
Yes, I mean automobile exhaust, campfire smoke, the second-hand industrial contaminants that confound so many cities, and the second-hand artificial smoke that my local barbecued ribs shop puts in their exhaust as advertising. Second-hand fumes are everywhere and it’s time to distinguish the harmful from the banal.
I have issues with the accompanying article primarily because it associates e-cigarettes and mental illness; this is a relationship I cannot fully support. Smoking tobacco has for centuries shown itself to be addictive but comforting. It has been a source of wealth and trade.
A break in battle.
It has been a symbol of friendship when communally consumed in a peace pipe, a calmative to soldiers suffering from the stress of battle, and to prisoners to counter the stress of captivity as well as a calmative for the mentally distressed.
In today’s anti-tobacco cultural wars little room is given to harm reduction because inhaling a misty vapor is conflated with harmful tobacco use. The truth is that the inhalation of a pure medication is superior to the natural tobacco product (CDC info). Harm reduction should be the aim and if nicotine has any benefits let’s provide it in the least harmful manner.
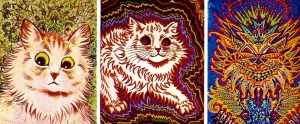
Cats painted over time of personality disintegration
– Carlos
Here’s Why We Should Give E-Cigarettes to Mentally Ill People
Yes, smoking can kill. It can also ease stress.
By Helen Redmond, March 19, 2014 | This article originally appeared in Substance.com:
“I want my cigarettes, I want my cigarettes, I want my cigarettes,” Charlie Cheswick, an enraged patient in a mental hospital, screams at the sadistically indifferent Nurse Ratched in the classic film One Flew Over The Cuckoo’s Nest. After several heartbreaking minutes, Jack Nicholson’s character, Randle P. McMurphy, breaks a window at the nursing station, grabs a carton of Marlboros and hands it to his deeply relieved comrade.
Gonzo author Thompson opining on life. – Carlos
The history of psychiatric hospitals is one of abuse, neglect and copious amounts of cigarette smoking. Until the 1970s, hundreds of thousands of mentally ill people were warehoused for decades in state mental asylums. There was typically little to do, and going to the supervised smoking room every 15 minutes became an “activity” to break the tedium. Cigarettes rewarded compliant behavior or were taken away to punish noncompliance. The scene from One Flew Over the Cuckoo’s Nest played out daily in hospitals nationwide.
That almost 90% of people diagnosed with schizophrenia smoke—despite tobacco’s well-known adverse health consequences—is a testament to the addictiveness of nicotine. But it is also evidence of nicotine’s power to chemically quell anxiety, depression and other upset. (The prevalence of smoking among people with bipolar and panic disorder, depression, anxiety and PTSD is also high.)
Hospital staff have long observed how smoking markedly improves the negative symptoms of mental illness, such as lack of motivation and pleasure, reduced emotional expression and deficits in attention and concentration.
“Whenever he runs out of cigarettes, he becomes highly agitated to the point where he has seriously injured staff and other patients. Providing a cigarette is generally much more effective at decreasing agitation than most medications I can provide,” Elizabeth Roberson, then a psychiatrist at Hawaii State Hospital, wrote to R.J. Reynolds in 2000, asking for free cigarettes for one of her patients.
The mentally ill remain the single-largest demographic of smokers, accounting for 44% to 46% of cigarettes sold in the US. This market earns the tobacco industry $37 billion annually. So it’s no surprise that the industry opposes smoking bans in psychiatric units. What may be surprising is that the National Alliance on Mental Illness (NAMI), a leading advocacy group for the mentally ill, collaborated with Big Tobacco in the 1990s to block smoking bans and to implement designated smoking areas. “It is inhumane to rob these patients of their autonomy and dignity by infringing on one of the few remaining freedoms historically allowed patients,” NAMI advocates said in 1995.
At the same time, the mentally ill also account for half of the estimated 400,000 Americans who die from a smoking-related health condition every year. The National Association of State Mental Health Program Directors reported in 2012 that people receiving public mental health services who have both an addiction and a mental illness die, on average, nearly 32 years earlier than others. Smoking is a major contributor to this premature mortality.
“The industry delivered carton-loads of cigarettes to psychiatric institutions. In some states, cigarettes were tax-free, “to be used for patient treatment.” R.J. Reynolds created “value” brands for “street people” and dispensed free samples to soup kitchens and homeless shelters.”
Given smoking’s many dangers and few benefits, for the “normal” person, whether or not to abstain is a no-brainer. But for the mentally ill, the risk/benefit analysis is more complicated. Their health-care providers know, on the one hand, that nicotine helps their patients cope with debilitating symptoms of mental illness and, on the other hand, that smoking causes fatal illness. The debate has polarized the mental health community. But the recent introduction of e-cigarettes—a safe nicotine-delivery device—has the potential to shift the terms of the debate.
Expected Benefits, Exaggerated Risks
Research over the past decade or so supports the view of nicotine as a potential therapeutic tool. It is both a stimulant and a relaxant. A drag on a cigarette sends nicotine from the lungs to the brain in under 10 seconds; once in the brain, it saturates the nicotinic receptors, triggering an instantaneous release of a host of neurotransmitters—acetylcholine, dopamine, endorphins, serotonin and glutamate—that improve mood, memory and concentration. Anxiety and pain are lessened.
Nicotine may even have specific properties that “treat” symptoms of schizophrenia. The drug helps to mitigate “sensory gating,” the ability to make sense of stimuli in the environment. When this function is impaired, as is often the case for schizophrenics, all sensory stimuli seem to be equally important, inducing confusion and fear in otherwise harmless situations. Gunvant Thaker, MD, the director of the schizophrenia-related disorders program at the Maryland Psychiatric Research Center, said, “When schizophrenic patients smoke, or are given nicotine gum, this deficit of sensory gating is reduced or normalized.”
Pharmaceutical companies are investing big bucks in the design and development of potential drugs with affinity for the brain’s nicotinic receptors—they mimic the action of nicotine itself—in order to package and sell these positive neurochemical effects.
Yet nicotine’s deadly connection to smoking tobacco has made it difficult to think rationally about nicotine as a stand-alone chemical. Anti-smoking advocates have also done their part to promote the misconception that nicotine is a dangerous drug with no therapeutic value. Yet the danger lies exclusively in the fact that as a vehicle to transport nicotine, tobacco has to be burned. When a cigarette is lit, the tobacco is transformed into tar and other carcinogens.
Pure nicotine, while addictive, is not dangerous, which is why the FDA has approved nicotine replacement therapies (NRT) like gums, patches, sprays and oral inhalation devices such as Nicotrol. Clinical and observational studies of NRTs have long shown that nicotine is a safe drug.
The Mentally Ill as a Major Market
Big Tobacco identified the mentally ill and the homeless as critical to their bottom line in the early 1970s when health warnings against smoking were first gaining wide acceptance. The industry quickly turned this marginalized group into a lucrative, loyal and captive market, according to the so-called Tobacco Papers, millions of the industry’s internal documents made public as a result of hard-won lawsuits in 1998.
The educated and affluent began to quit in large numbers. The social acceptability of smoking waned and new restrictions on smoking prompted still more quitting. The customer loss cut into profit margins, and tobacco companies sought to reinforce marketing to the mentally ill and the homeless (two thirds of the severely mentally ill are homeless or at risk). The industry delivered carton-loads of cigarettes to psychiatric institutions. In some states, cigarettes were purchased tax-free and were “to be used for patient treatment.” R.J. Reynolds created “value” brands for “street people” and dispensed free samples to soup kitchens, homeless shelters and homeless service organizations.
The Tobacco Papers document the beleaguered industry’s many efforts to make the most of this market. Philip Morris ran an ad for Merit cigarettes that seemed to many mental health professionals to be targeted to schizophrenics themselves. The ad showed a double image of a pack of Merits and read, “Schizophrenic…For New Merit, having two sides is just normal behavior.”
Eager to “find” benefits of cigarettes, Big Tobacco left no stone unturned in funding research. A well-paid British psychiatrist promoted the idea that heavy-smoking schizophrenics were less susceptible to lung cancer. This notion was debunked only in the late 1980s.
Other research focused on the idea that the mentally ill were smoking to “self-medicate.” John A. Rosecrans, a psychopharmacologist currently at Virginia Commonwealth University, did industry-funded work on the therapeutic effects of nicotine for people with schizophrenia, anxiety and depression, ADHD and other neurological conditions. “The future for developing nicotine as a therapeutic agent…using a safe delivery system is relatively good,” he concluded. “One of the difficulties with a chemical such as nicotine is that it has been thought of as a ‘dirty drug’ or ‘demon drug’ like heroin, which makes people addicts. We first need to pull away from this concept of demonism and treat nicotine and its analogues like any other drug.” Rosecrans’s research was not based on junk science. Now, 16 years later, the nicotine’ potential benefits is being studied in all of the diseases he listed.
Will E-Cigarettes Change the Game?

Not tobacco smoke, mist
The introduction of the e-cigarette dramatically alters the risk/benefit equation of nicotine by dramatically cutting the rate of smoking-related disease and death. The battery-powered device looks like a cigarette and is activated by drawing on the mouthpiece (like on a cigarette). A liquid nicotine cartridge is heated and turned into vapor, which is inhaled. There is no tobacco and no combustion.
Opponents of e-cigarettes say that they pose safety concerns, especially because the FDA does not currently regulate them.
But studies conducted in Japan, Italy and the US suggest that e-cigarettes are a safe way to deliver nicotine. “Retailers all over the world have already sold millions of electronic cigarettes, yet there is no evidence that these products have endangered anyone and no indication that electronic cigarettes are any more of an immediate threat to public health and safety than traditional cigarettes,” the researchers of one study concluded. “E-cigarettes appear to be much safer than tobacco cigarettes and comparable in toxicity to conventional nicotine-replacement products.”
“Smoking provides “cover rituals for patients having psychiatric symptoms,” said a psychiatric hospital director. “You tamp the box, you play with the lighter, you can exhale and look into the middle distance and not look like you’re hallucinating.” E-cigarettes preserve these rituals.”
For smokers, the rituals of smoking are as powerful as the hit of nicotine: lighting the cigarette, the inhalation and exhalation of smoke, tactile and oral sensations. Nicotine patches, gums, sprays and medications eliminate these ritualistic aspects, and this may contribute to their high failure rates. For the mentally ill, smoking rituals help focus attention on one thing, alleviate boredom and experience pleasure. Socially, smoking provides “cover rituals for patients having psychiatric symptoms,” said Rona Hu, medical director of the acute psychiatric inpatient unit at Stanford Hospital. “You tamp the box, you play with the lighter, you can exhale and look into the middle distance and not look like you’re hallucinating.” E-cigarettes, because they preserve these rituals, may be more likely to be used consistently than other NRTs.
But anti-smoking advocates have mounted an effective campaign against electronic cigarettes. The response by CASAColumbia, an addiction and substance use think-tank affiliated with Columbia University, to e-cigarettes is representative of the advocates’ abstinence-only approach. In “E-cigarettes Seem to Be a Bad Idea No Matter How You Cut It,” CASAColumbia states its opposition to “the unregulated production, promotion and selling of e-cigarettes.”
CASAColumbia argues that nicotine is harmful simply because it is addictive. (The same can be said of caffeine, but there is no comparable campaign against coffee.) Its main argument is that young people could use them “as a bridge to other addictive substances including conventional cigarettes.” The group concedes that vaporized nicotine “could have therapeutic value,” but only if used for the purpose of complete nicotine cessation. There is no mention of the numerous, well-documented positive effects of nicotine.
David Nutt, the director of neuropsychopharmacology at Imperial College London and a former drug advisor to the British government, has endorsed e-cigarettes. “I’m totally in favor of this kind of harm reduction approach,” he said. “Electronic cigarettes should not be controlled as medicines—they should be controlled more lightly than cigarettes in order to encourage people to switch.”
Organizations that support the mentally ill remain on the fence. The National Alliance on Mental Illness’s director of media relations, Bob Carolla, said, “NAMI doesn’t have a position on electronic cigarettes. We are studying the issue and consulting with experts in the field.”
The FDA is in the process of making a ruling about how to regulate e-cigarettes, according to a January 2014 announcement. Mitch Zeller, the director of the Center for Tobacco Products, is reportedly meeting with e-cigarette manufacturers to gather data.
It is my view that, based on the well-established principles of harm reduction, e-cigarettes should be available to help smokers reduce their risk. They can also serve as a new approach to maintaining nicotine addiction, like methadone maintenance or buprenorphine for opiate dependency. Nicotine cartridges come in different strengths with which to taper down or quit.
For smokers who have chronic mental illness, the case for nicotine maintenance via e-cigarettes is even more powerful. Many are simply unable to remain completely abstinent. In a current JAMA study, Harvard researchers report that the decline in smoking, from 2004 to 2011, among people with mental illness was significantly less (from 25.3% to 23.8%) than among those without mental illness (from 19.2% to 16.5%). This is not only because of nicotine’s addictiveness but also because of its significant therapeutic benefits. Health-care providers should encourage their mentally ill patients to switch to e-cigarettes; psychiatric facilities should make them widely available and provide space for their use.
More research is needed on the long-term effects and safety of e-cigarettes. But we cannot wait indefinitely—until all the scientific evidence is in—while hundreds of thousands of people remain at high risk simply because they cannot, or do not want to, achieve total abstinence. Close to half of these people are mentally ill, a group for whom cigarette smoking has a special significance. It is unethical to deny them access to a nicotine delivery device that could save their lives.
18 COMMENTS
Helen Redmond is a freelance journalist and a drug and health policy analyst.